

The Perils of Advanced Prostate Cancer Therapy - 018
The Perils of Advanced Prostate Cancer Therapy - 018
Prolonging life but at a cost

One of the most disturbing things I’ve learned about advanced prostate cancer therapies is that the drugs used to treat it usually can’t cure you and also cause your cancer to become more aggressive.
In addition, common side effects of these drugs include:
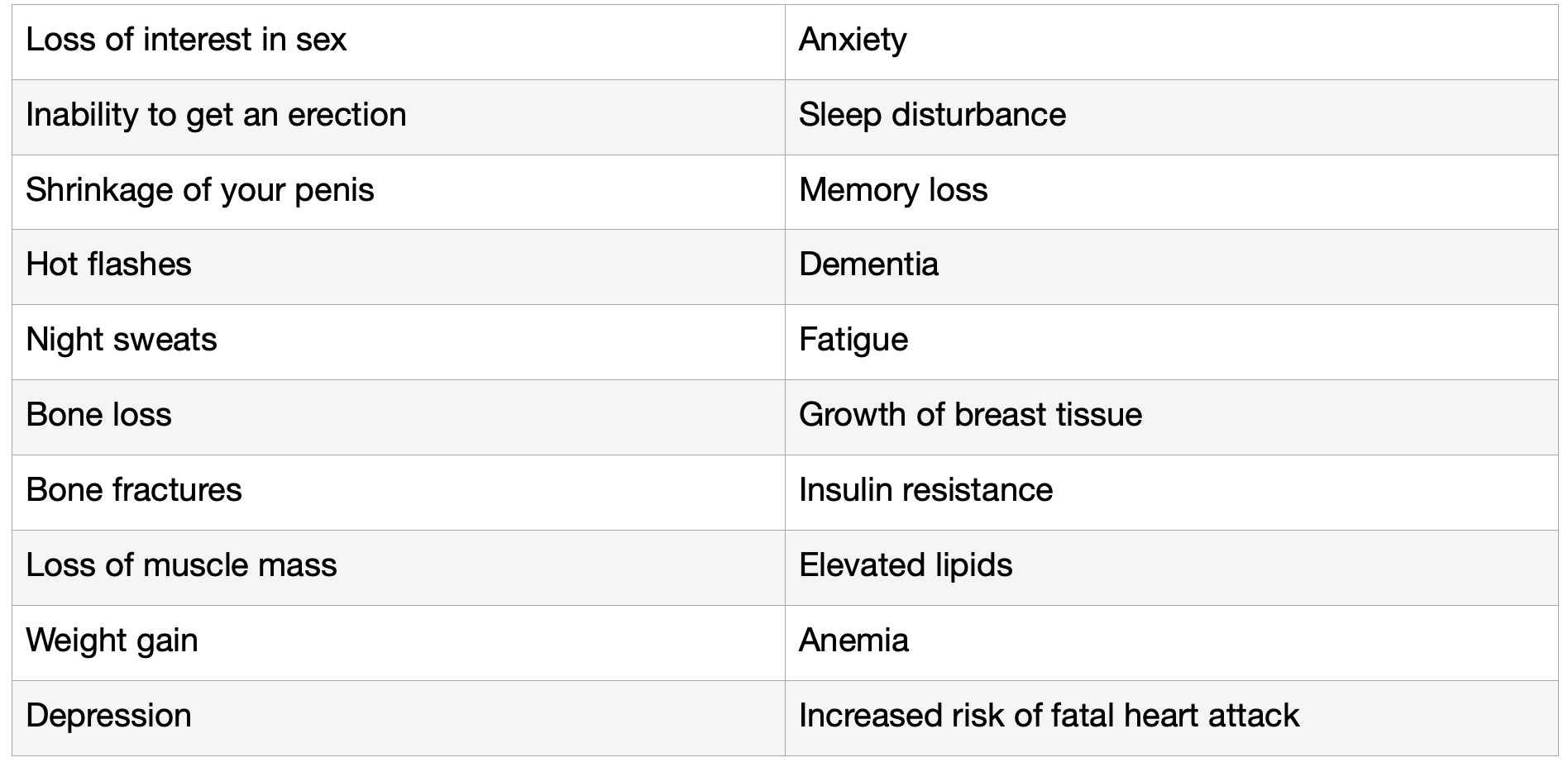
The main treatment for advanced prostate cancer involves either reducing or blocking androgens, typically testosterone and dihydrotestosterone, but this approach rarely results in a cure. And there’s scientific evidence that in many men, these drugs mutate the tumor into more aggressive tumor types.
In 1966, a physician, Charles Huggins, won “The Nobel Prize in Physiology of Medicine” for his work showing that some cancers responded to hormonal manipulation. In 1940, he announced that prostate cancer responded to the removal of the testicles (castration) or the administration of estrogen. Since testosterone fuels prostate cancer growth, he found that by removing the testicles, which are the main source of testosterone, you could put patients into prolonged remission and even cure those with organ-confined or early disease.
At the time, this was a dramatic breakthrough in cancer therapy. But more than eighty years later, androgen deprivation therapy (ADT) and newer drugs called androgen receptor signaling inhibitors remain the mainstay of prostate cancer treatment. This is despite clinical studies proving that drugs that lower and inhibit the production of testosterone play a direct role in mutating prostate cancer into more aggressive variants.
Part of the problem is that cancer drugs that work by modulating the immune system, called immunotherapy, don’t work as well for prostate cancer as in other types of immunologically “hot” cancers. Immunologically “hot” tumors tend to have a more inflamed microenvironment with a lot of T-cell infiltration. This is relatively rare in prostate cancer, and the majority of prostate cancers are considered “cold” tumors and thus not responsive to immunotherapy.
Because of this, the pharmaceutical industry has mostly continued to focus on producing drugs that inhibit the production of androgens or block androgen receptors. So why do pharmaceutical companies continue to focus on developing very expensive drugs for advanced prostate cancer that will never lead to a cure and mutate the tumor? Because they know that treatment of advanced prostate cancer is currently a no-win situation and that the Food and Drug Administration (FDA) will approve drugs that only extend overall survival by two to four months!
By “no-win,” I mean that for most men with advanced prostate cancer, treatment is considered palliative and not curative. And because doctors are so desperate to say they have a drug that will increase your survival time in an incurable disease, they will prescribe expensive drugs that ironically have life-threatening side effects.
Desperate times call for desperate measures!
Advanced prostate cancer is an extremely heterogeneous cancer, meaning it is highly variable from individual to individual, and you can have multiple tumor types within the same person. That variability is what results in one man having an extremely slow-growing cancer to another dying from it within months.
It’s tricky in that some men who thought they were cured after having their prostates removed or radiated go on to develop a recurrence of the tumor ten years later. Scientists attribute that to dormancy, where cancer cells go into a dormant state, or hibernation, only to emerge years later and wreak havoc.
Reasons for the heterogeneity of advanced prostate cancer are multifactorial, and genetic mutations play a role. Genetic mutations triggered by the drugs themselves help create resistance to the drugs used to treat it. It’s like a snake eating its tail but gives the snake a much longer time to eat itself.
Most men with advanced prostate cancer don’t know that many published studies show that androgen deprivation therapy (ADT), which lowers testosterone, produces “selective pressures” in the body to create more aggressive tumor types, which increases the risk for metastases.
In my experience, not a single physician discussed this risk with me when recommending I start ADT unless I brought up the subject. Even then, some tried to downplay it by saying that men with advanced prostate cancer also develop resistance to chemotherapy and radiation. One of the physicians went on to describe this process as simply tumors outsmarting the treatment as if it’s some type of passive process that has more to do with the intelligence of the tumor than a problem with the drugs themselves.
A simplified description of the progression of prostate cancer tumor types is that prostate cancer typically starts as castrate-sensitive. Castrate-sensitive, also called hormone-sensitive prostate cancer responds to the lowering of testosterone levels by either removing a man’s testicles (orchiectomy) or using androgen deprivation therapy (ADT) drugs to lower testosterone to less than 50 ng/dL and preferably less than 20 ng/dL.
Testosterone, an androgen, fuels prostate cancer, and by reducing its fuel, you’ll typically see a disappearance of the tumors and a lowering of tumor marker prostate-specific antigen (PSA) levels. But in advanced prostate cancer, where cancer has spread outside the prostate gland, this response is relatively short-lived.
When prostate cancer grows, and the PSA level rises despite castrate levels of testosterone, the tumor type is now called castrate-resistant, also known as hormone-resistant. The tumor has found a way to thrive and grow either by using other fuel sources or by thriving off lower levels of testosterone, typically a combination of both.
Disease progression from castrate-sensitive to castrate-resistant typically occurs at a median of 18–24 months after beginning ADT despite maintenance of castrate testosterone serum levels of less than 20 ng/dl.1 When castrate-sensitive prostate cancer (CSPC) transforms into castrate-resistant prostate cancer (CRPC), it becomes more aggressive and harder to treat.
In addition, some of the drugs used to treat castrate-resistant prostate cancer (CRPC) lead to tumor mutations that result in an even more highly aggressive tumor called treatment-emergent neuroendocrine prostate cancer (T-NEPC). Neuroendocrine prostate cancer not caused by treatment is very rare and accounts for less than 2% of all prostate cancers.
However, treatment-emergent neuroendocrine prostate cancer is much more common. One study showed that in an evaluation of 231 cases of castrate-resistant prostate cancer that had undergone treatment, a whopping 40.7% of these on repeat biopsy after treatment were found to have developed treatment-emergent neuroendocrine prostate cancer.2
T-NEPC is an aggressive variant of castrate-resistant prostate cancer and has an abysmal prognosis. Most T-NEPC patients die within 1 to 2 years after diagnosis, accounting for approximately 25% of CRPC deaths.3
The very first scientific article I stumbled upon in researching treatment-induced resistance is appropriately titled Androgen deprivation of prostate cancer: Leading to a therapeutic dead end.4 This journal article was published in 2015 with its main points being:
Androgen deprivation therapy (ADT) leads to numerous molecular alterations in prostate cancer.
ADT promotes more aggressive behavior and metastasis of tumor cells.
ADT ends in incurable castration-resistant disease.
ADT of advanced prostate cancer leads to a reduced efficacy of anticancer agents.
Therapeutic intervention seems to be indicated before castration resistance occurs.
What the authors meant by the last bullet point is that scientists and doctors should design more clinical trials that incorporate other types of therapies besides monotherapy with ADT for castrate-sensitive prostate cancer. Thankfully, these types of clinical trials have increased since 2015, and some have shown promising results.
For example, triplet therapy with the oral androgen receptor inhibitor darolutamide plus docetaxel (chemotherapy) plus androgen-deprivation therapy significantly improved overall survival in patients with metastatic hormone-sensitive prostate cancer vs docetaxel plus androgen-deprivation therapy in the phase III ARASENS trial.5
Despite the improvement in overall survival using newer combination therapies in castrate-sensitive prostate cancer, what didn’t change was the other main points made by the authors. Triplet therapy still resulted in molecular alterations in prostate cancer, which promoted more aggressive behavior and metastases of tumor cells, eventually ending in incurable castrate-resistant disease. Triplet therapy in castrate-sensitive prostate cancer increased overall survival time but only delayed the inevitable.
In addition, triplet therapy increases the side effects of the various drugs being used. You now have to worry about experiencing side effects from not one drug but three. Some would say, “Yes, but it gave men more time before dying.” My answer is, “Yes but triplet therapy still results in a therapeutic dead end.” Despite this improvement in overall survival, we are still a long way away from finding therapies for advanced prostate cancer that result in durable remissions and cures.
Physicians who treat advanced prostate cancer have become so desperate for effective therapies that some drugs approved by the FDA increase overall survival by only four months. Such is the case with the 2010 approval of Sipuleucil-T, a recombinant antigen protein that must be incubated with the patient’s white blood cells.
This mixture is infused back into the patient as a vaccine and is thought to cause a release of immune modulators called cytokines in an attempt to destroy the tumor cells. The vaccine is infused every two weeks for sixty minutes in three doses. In 2011, the cost of the treatment was $93,000, equating to $22,683 per month for the extra four months of life. In 2019, the wholesale cost of treatment with Sipuleucil-T was $133,000. Desperate times call for desperate measures.
Aside from prostatectomy, radiation, and ADT, it is only in the past 18 years that other types of drugs have been approved for the treatment of prostate cancer. Despite these newer therapies, advanced prostate cancer continues to mutate into more aggressive forms as therapy progresses.
Some tumors are found to have primary resistance to these types of newer drugs, meaning they were resistant to these drugs even before being treated with them. But multiple studies suggest that resistance arises as a result of exposure to these newer potent androgen signaling inhibitor drugs.6 7 8
Aggressive tumor types may exist in certain individuals even before receiving any treatment. However, the medical literature indicates that treatment-induced mutations from less aggressive to more aggressive tumor types occur in a majority of advanced CRPC patients who have been treated with androgen-inhibiting drugs.
I’m writing this article to create awareness for patients and doctors around this very concerning issue. We must continue to support organizations such as the Prostate Cancer Foundation that raise awareness and funds to support innovative prostate cancer research that has nothing to do with androgen inhibition. Funding by the Prostate Cancer Foundation played a major role in supporting research that helped get prostate-specific membrane antigen radioligand therapy (PSMA RLT) FDA-approved.
Some will argue that my concern with ADT and androgen-inhibiting drugs is not well-founded based on the significant increase in overall survival of patients getting triplet therapy with novel drugs such as darolutamide. My response is that until researchers can figure out how to block or reverse the creation of these drug-induced mutations, more emphasis should be placed on future prostate cancer therapy research that doesn’t involve androgen deprivation and androgen inhibition.
Keith R. Holden, M.D.
W.P. Harris, E.A. Mostaghel, P.S. Nelson, B. Montgomery. Androgen deprivation therapy: progress in understanding mechanisms of resistance and optimizing androgen depletion. Nat. Clin. Pract. Urol, 6 (2) (2009), pp. 76-85
Zhang, Q., Han, Y., Zhang, Y., Liu, D., Ming, J., Huang, B., & Qiu, X. (2001, January 1). Treatment-Emergent Neuroendocrine Prostate Cancer: A Clinicopathological and Immunohistochemical Analysis of 94 Cases. Frontiers; https://www.frontiersin.org.articles/10.3389/fonc.2020.571308/full#B1
Conteduca V, Oromendia C, Eng K, Bareja R, Sigouros M, Molina A, et al. Clinical features of neuroendocrine prostate cancer. Eur J Cancer (2019) 121:7–18. doi: 10.1016/j.ejca.2019.08.011
Katzenwadel, A., & Wolf, P. (2015). Androgen deprivation of prostate cancer: Leading to a therapeutic dead end. Cancer Letters, 367(1), 12-17. https://doi.org/10.1016/j.canlet.2015.06.021
Smith M, Hussain MHA, Saad F, et al: Overall survival with darolutamide vs placebo in combination with androgen-deprivation therapy and docetaxel for metastatic hormone-sensitive prostate cancer in the phase 3 ARASENS trial. 2022 ASCO Genitourinary Cancers Symposium. Abstract 13. Presented February 18, 2022.
Aggarwal R, Huang J, Alumkal JJ, et al. Clinical and genomic characterization of treatment-emergent small-cell neuroendocrine prostate cancer: a multi-institutional prospective study. J Clin Oncol. 2018;36:2492-2503.
Bluemn EG, Coleman IM, Lucas JM, et al. Androgen receptor pathway-independent prostate cancer is sustained through FGF signaling. Cancer Cell. 2017; 32:474-489.e6.
Abida W, Cyrta J, Heller G, et al. Genomic correlates of clinical outcome in advanced prostate cancer. Proc Natl Acad Sci USA. 2019;116:11428-11436.