

Oligometastatic Prostate Cancer - 020
Oligometastatic Prostate Cancer - 020
Exploiting this scenario for a cure

I’ll start with a quick recap. I was diagnosed with prostate cancer in December 2017 and underwent surgical removal of my prostate in April 2018, which found cancer in two of my pelvic lymph nodes. I was intolerant of androgen deprivation therapy (ADT) to lower testosterone, which is a hormone that feeds prostate cancer. I underwent radiation therapy to my pelvis from August through November 2018. In January 2019, my prostate-specific antigen (PSA) tumor marker had dropped from a postoperative level of 4.8 to 0.9. If surgery or radiation had cured me, my PSA would have been zero.
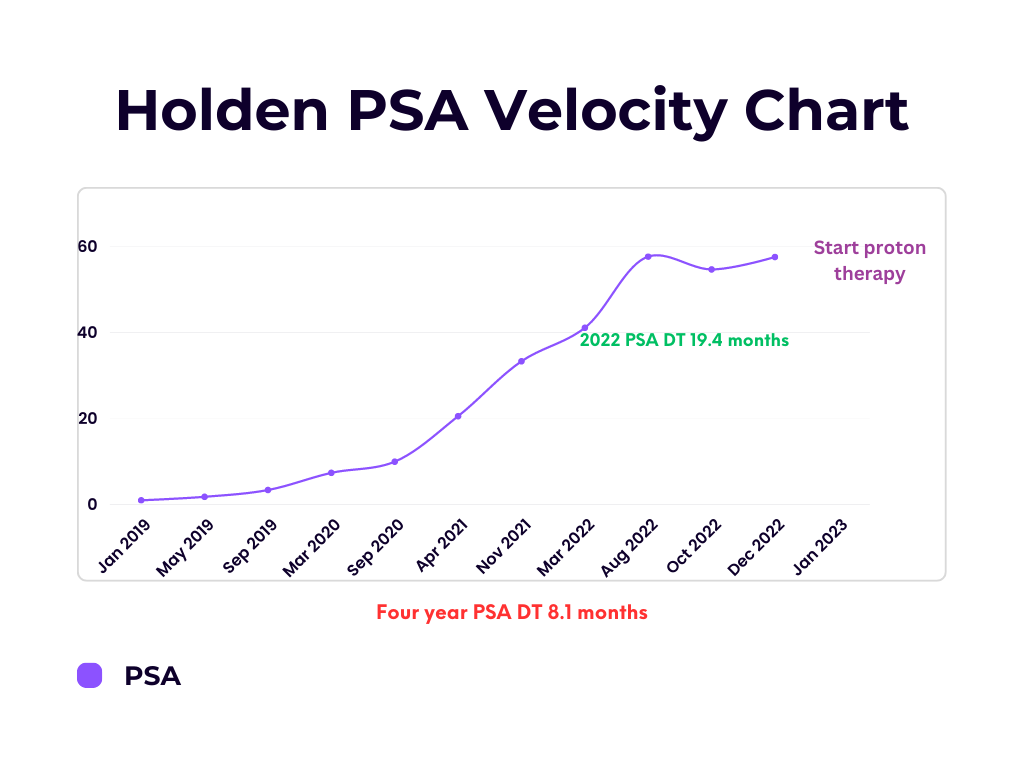
I kept a chart measuring how fast my PSA level doubled for the next four years. This is also known as the PSA doubling time (DT), which indicates the rate of tumor growth. A DT of fewer than 10 months generally indicates aggressive cancer, while a DT of more than 24 months may suggest slow-growing cancer.
The miracle I referenced in the last newsletter is the plateau in the velocity curve from August 2022 through January 2023. The even bigger miracle is that my PSA dropped from 57.7 on August 1, 2022, to 54.7 on October 12, 2022! The only previous time my PSA had dropped was when I was in traditional medical therapy. This drop and plateau of my PSA indicate that the cancer had significantly slowed its growth and may even have stopped growing for some time.
This PSA stall was also reflected in serial positron emission tomography (PET) scans taken during that time. Hallelujah! What caused this? We’ll never know for sure, but during that time, I was doing only all-natural remedies.
I don’t think it’s a coincidence that the PSA stall started around the time Mike and I took a two-week trip to Europe and had one of the best vacations of our lives. Most days while on vacation I never thought about having prostate cancer and transported my mind and body into a time and place without cancer.
Never underestimate the power of the mind over the body, especially when it comes to stress reduction.
As my PSA velocity chart shows, over the 4 years from January 2019 to January 2023, my overall PSA doubling time was 8 months - not good. But during 2022, my PSA doubling time slowed to 19 months - fantastic! Now there is a caveat to this discussion of a slowing PSA DT, meaning that prostate cancer growth is slowing.
Some men with aggressive types of prostate cancer may have a low PSA of, say, 1.9 and have metastatic cancer lesions all over their bodies. This is especially true with neuroendocrine prostate cancer tumors because these aggressive tumors have morphed into tumors that have lost their ability to produce PSA. These aggressive prostate cancer cells no longer resemble prostate cells.
In addition to the natural remedies, I had started taking Mondays off work and was getting more rest. Because of that, I was exercising regularly - weight training on the weekends and walking on weekdays. Several studies show that regular exercise increases overall survival in prostate cancer.
Kenfield, S. A., Stampfer, M. J., Giovannucci, E., & Chan, J. M. (2011). Physical Activity and Survival After Prostate Cancer Diagnosis in the Health Professionals Follow-Up Study. Journal of Clinical Oncology, 29(6), 726–732. https://doi.org/10.1200/jco.2010.31.5226
Oligometastatic disease
Most promising was that serial PET scans suggested I had a subtype of cancer called oligometastatic prostate cancer. Oligometastatic prostate cancer is a subtype of metastatic prostate cancer characterized by a limited number of metastatic lesions, usually defined as three to five. My serial scans showed I had approximately six lesions in the lymphatic chains lining both sides of my descending aorta from just below my diaphragm to the top of my pelvis.
Patients with oligometastatic prostate cancer tend to have a better prognosis than those with widespread metastases, and this subtype can be managed with metastasis-directed therapy (MDT). My radiation oncologist and I decided we were going to attempt to exploit this oligometastatic disease state and go after the six visible metastatic lesions with radiation therapy.
Metastasis-directed therapy
Metastasis-directed therapy (MDT) refers to any local therapy that targets metastases in specific sites, including surgery or radiation. The goal of MDT is to eradicate all visible sites of cancer and thereby delay the progression of the disease, produce a durable remission, and even cure some cancers.
The development of trials and identification of patients who would benefit from MDT are currently limited by a simplistic definition of oligometastasis and minimal understanding of what drives metastatic biological potential.
Beckham, T. H., Yang, T., Gomez, D. R., & Tsai, C. (2021). Metastasis-directed therapy for oligometastasis and beyond. British Journal of Cancer, 124(1), 136–141. https://doi.org/10.1038/s41416-020-01128-5
The rationale behind MDT is that if a patient's disease is controlled, it may delay or prevent their need for systemic therapy, such as androgen deprivation therapy (ADT), which can have life-threatening side effects.
The perils of androgen deprivation therapy (ADT)
In my case, ADT wasn’t an option as just two months of it had caused me intolerable side effects. And as I’ve discussed previously, there is scientific proof that ADT mutates prostate cancer into a more aggressive tumor called hormone-resistant prostate cancer (HRPC).
That statement is considered controversial among physicians who treat advanced prostate cancer. They know some studies show ADT prolongs overall survival and even cures some men with advanced prostate cancer. But for advanced prostate cancer, ADT alone is not considered the standard of care. ADT is supposed to be combined with surgery, radiation, and other drugs.
The problem is that prostate cancer is a very heterogenous type of cancer, varying from man to man and even manifesting as multiple types of prostate cancers in the same man. There is no way to know exactly which individual man will benefit from ADT and who will not. The studies that show improved survival in men treated with prostate cancer also include men who died fairly early while on ADT.
There are multiple papers written on how participants in most clinical trials don’t reflect real-world samples of men. Clinical trials allow you to cherry-pick the men who you’ll let into your study by creating inclusion and exclusion criteria. Since the vast majority of clinical trials are designed and funded by pharmaceutical companies testing their drugs, they want to cherry-pick the men into their trials who they think may benefit the most.
Even then, there are many men in these trials who die comparatively early when treated with ADT. Part of this is because ADT mutates tumors and has numerous life-threatening side effects, especially in men with coronary artery disease and vascular disease.
I’m an example of an anomalous type of prostate cancer patient. It’s been 6 years and 2 months since I was diagnosed with advanced prostate cancer. I consider it a blessing in disguise that I wasn’t able to tolerate ADT and only took two months of a long-acting injection of the drug. Because I wasn’t on ADT long enough to see a rise in my PSA while on therapy, which would reflect the development of mutations, I’m still considered to have hormone-sensitive prostate cancer (HSPC).
In addition, the prostate cancer in my body is a mixed bag of quandaries. Despite no traditional medical therapies in just over 5 years and an overall doubling time of 8 months, I strangely have no detectable bone metastases despite undergoing multiple types of bone and PET scans. Typically the first place prostate cancer metastasizes to is bone. Also, there’s the unexplained plateau in the growth of the cancer reflected by my PETS scans and PSA levels.
In keeping with this anomalous presentation, I have worked my ass off to do everything in my power to cure this cancer from a lifestyle and nutrition standpoint. I’ll save those details for another newsletter since the list is quite long.
Had I stayed on ADT, there is a high likelihood that by now, I’d have hormone-resistant prostate cancer (HRPC) - a mutated and more aggressive cancer that has learned to grow without testosterone or with less testosterone. Even though newer therapies can prolong survival in some men with advanced HRPC, this requires layering multiple drugs and adding chemotherapy, exponentially increasing the risk of severe side effects.
Deciding which metastasis-directed therapy
Surgery wasn’t an option as there were too many lymph nodes on both sides of my aorta. Too dangerous. So what’s left? Radiation. There are multiple types of radiation. I had already undergone 8 weeks of intensity-modulated radiation therapy (IMRT) to my pelvis in the fall of 2018. IMRT allows for computer-adjusted doses and fields of radiation treatment. I had already decided against IMRT this time because, in my mind, it provides the least focused treatment field, considering the other two types of radiation I was considering.
It was about this time that my original radiation oncologist, Dr. Scot Ackerman, hired a new physician for his clinic. His name is Jaymeson Stroud, M.D. He is a very intelligent and kind physician who was chosen as Chief Resident of his radiation oncology program at Washington University in Saint Louis, MO. When I first met Dr. Stroud, it was similar to meeting Dr. Ackerman. I immediately felt comfortable and felt like I knew him. It’s hard to describe.
Stereotactic body radiation therapy (SBRT)
I told Dr. Stroud that I wasn’t interested in another round of IMRT and that I had read about using stereotactic body radiation therapy (SBRT), also known as stereotactic ablative radiotherapy. SBRT is a type of radiation therapy that delivers super high doses of radiation to a precise target in the body. The radiation is delivered from different angles, and the beams converge at the target. This high-precision radiation technique minimizes damage to surrounding healthy tissue and allows for a higher radiation dose to be delivered to the tumor. SBRT is typically delivered in 1-5 treatments.
He then suggested we use proton therapy. His rationale was that he had participated in many online physician forums with other radiation oncologists who observed that when SBRT was used in lymph node metastases, tumors in nearby lymph nodes often recur. Despite the data supporting using SBRT for MDT, Dr. Stroud was thinking out of the box and using his gut feeling based on real-world feedback from fellow radiation oncologists. I like that trait in my physicians.
This idea makes sense since the lymph chains are connected like the limbs of a tree. In addition, the cancer in my lymph nodes seemed to be confined to the lymph chains on both sides of my aorta though spread out from the top of my pelvis to the bottom of my diaphragm. Surely there were some micrometastases hiding in these lymph chains that weren’t lighting up on PET scans.
Dr. Stround smartly recommended we use proton therapy to “paint” the lymph chains and deliver extra focused doses to “boost” the lymph nodes that were lighting up with cancer. That way, we were more likely to get all of the tumor cells. Brilliant! We would use proton therapy for my MDT. I felt really good about this decision.
I was lucky enough that Dr. Ackerman, a pioneer, had invested in building a 30 million-dollar proton therapy machine in 2015 when the therapy was fairly new to insurance companies and clinical trials. Dr. Ackerman’s proton machine now runs from early morning to late at night, helping many men and women fight various types of cancers. There are only 41 proton centers in the United States, and about 20 states don’t even have a proton therapy center. Here is a link to a map of proton centers in the U.S.
Proton therapy
Proton therapy is different from conventional radiation therapy in that it uses positively charged high-energy proton particles to target cancer cells with high precision. Proton therapy works by using a machine called a cyclotron to accelerate protons to very high speeds. These protons are then directed through a beamline to a treatment room, where the patient is positioned on a treatment table.
The beam of protons is directed to the tumor site, where the positively charged protons interact with negatively charged electrons in the cancer cells, causing damage to the DNA of the cells. This damage prevents the cancer cells from dividing and growing, ultimately leading to their death.
One of the key benefits of proton therapy is its ability to target cancer cells with precision while minimizing damage to surrounding healthy tissue. This is achieved by adjusting the proton beam's energy so that it deposits its maximum energy at the tumor site, called a Bragg peak, sparing healthy tissue beyond the tumor.
Another benefit of proton therapy is that it can be used to treat tumors that are resistant to conventional radiation therapy. This is because proton particles can be delivered to the tumor site at a higher dose than conventional radiation, allowing for greater damage to cancer cells.
Conclusion
Although I couldn’t find any completed clinical trials that used proton therapy to treat oligometastatic prostate cancer, the data coming from trials using SBRT is extremely promising. As I have done during this entire journey, I defaulted to what my medical training and gut told me. And in this instance, I feel that Dr. Stroud and I have made the right decision to go with proton therapy. He made that suggestion even though we could have done SBRT in his office.
Since my diagnosis, my gut decisions and really talented physicians have led me to a place where I am doing quite well despite 5 years without traditional therapy. So here we go again, this time with proton therapy. Time will tell if we made the right decision.
In the next newsletter, I’ll explain why the prior diagnosis of a metastatic lesion in my prostate bed on an Axumin PET scan was an error. Until then, stay positive and stay strong.
Much love,
Keith R. Holden, M.D.
Stay strong and keep pushing the envelope!