

Prostate Cancer Secrets

This is Prostate Cancer Secrets, a newsletter written by a physician with advanced prostate cancer. I’m writing this newsletter to educate people, including doctors, about advanced prostate cancer.
Advanced prostate cancer is prostate cancer that has left the confines of the prostate gland. Prostate cancer is a cancer of extreme duality in that the vast majority of men diagnosed with prostate cancer are caught early before it has left the prostate gland, and most of those are curable. But once it leaves the prostate gland, advanced prostate cancer is considered incurable except for the very few men who are considered outliers.
Outliers are men with advanced prostate cancer who defied the odds and go into what is termed “durable remission” or “spontaneous remission.” But because I’ve been diagnosed with advanced prostate cancer with lymph node metastases, science isn’t going to save me. Meaning the medications used to treat advanced prostate cancer haven’t been shown to cure prostate cancer, only to prolong lives. That is unless you are the rare outlier, but even then, doctors can’t say definitively that the medication cured them. Doctors never say “cure” regarding advanced prostate cancer, but will call it a “durable remission” when a man is an exceptional responder to therapy.
Durable remission is rare and usually doesn’t last. Durable remission usually just means these men live longer than expected, but eventually die of prostate cancer. This is different from spontaneous regression or spontaneous remission, which can occur when there has been no therapy at all despite having advanced prostate cancer. I have found only one example of this in the medical literature and it was ironically a physician whose cancer disappeared without therapy after metastasizing to the lymph nodes. I call spontaneous remission a miracle, and thankfully, no one is immune to miracles.
I underwent a radical prostatectomy (removal of my prostate) in April of 2018. Pathology from my surgery showed cancer had invaded the local tissue surrounding my prostate and had spread into my pelvic lymph nodes. Pathology margins were positive, meaning cancer cells were left behind. My Gleason score was 4 + 3 = 7, which is considered unfavorable and high risk for recurrence and metastases. Unfortunately, the surgical pathology also showed I had a small portion of Gleason grade 5 cells present, which raised my risk even higher. Gleason grade 5 prostate cancer cells have mutated so much that they hardly resemble normal prostate cells and confer the highest risk of all.
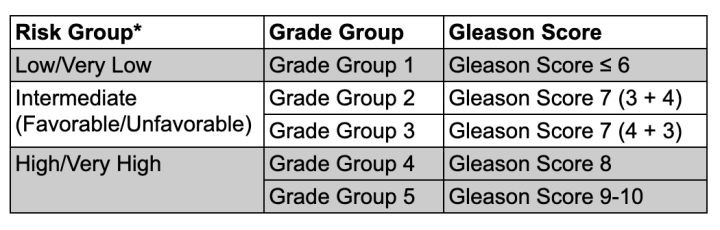
*Risk Groups are defined by the Grade Group of the cancer and other measures, including PSA, clinical tumor stage (T stage), PSA density, and number of positive biopsy cores.
Click here for more information about the Gleason score.
I went on to try androgen deprivation therapy, which is medication used to decrease my testosterone as low as possible. This is because, in general, testosterone feeds prostate cancer cells, though there are a few exceptions, which I’ll go into in a later newsletter.
I only tolerated two months of testosterone lowering therapy before I had to stop it because of terrible side effects. I also underwent eight weeks of radiation to my prostate bed and whole pelvis, which also caused severe side effects. My PSA (prostate cancer tumor marker) never dropped to undetectable and has been steadily rising since surgery and radiation. Because I can’t tolerate testosterone lowering therapy, which is the primary treatment for advanced prostate cancer, it’s going to be up to me at this point, not science, on how long I live.
Despite all that has happened, I still have a positive mindset, which is key to prolonging my survival. In fact, it’s probably the key issue if I’m to be an outlier and go into spontaneous remission. If the other physician did it, why can’t I?
So this newsletter will take you along on my journey from the very beginning when my symptoms first started until now. I’ll detail some surprising things I learned along the way, and hopefully, entertain you with some amazingly positive experiences I’ve had. Some of the experiences can only be considered what my Dad called “God-incidents.” I call them synchronicities. One benefit of having cancer is that my spirituality has grown in amazing ways as I’ve progressed along this journey.
I want to show people that they can face something terrible and still find peace and joy in their life. Most importantly, I want to show you how to maintain hope in the face of fear and uncertainty.
Another reason for writing this newsletter is to educate doctors who treat people with cancer. This is because I’ve had some shockingly horrible experiences with some doctors along the way. Mostly those experiences were due to poor bedside manner and lack of knowledge about the nocebo effect.
In addition, because advanced prostate cancer is so complex, many physicians, even the ones who treat it, don’t know the rapidly changing standard of care for treating it. And this is why you’ll see me recommend every man with advanced prostate cancer get at least one consultation with a physician in an academic institution considered a prostate cancer center of excellence.
Advanced prostate cancer is super complex:
1) It is highly heterogenous with multiple tumor types even in the same individual.
2) A super-intelligent cancer that undergoes some incredible mutations to survive. It can form BRCA mutations like those with breast and ovarian cancer even if that’s not in the family bloodline.
3) It forms highly aggressive mutations directly due to the medications used to treat it. One specific mutation turns one of the medications (bicalutamide) used to treat it from a testosterone receptor blocker to a testosterone receptor promoter. Meaning the drug starts to promote prostate cancer growth!
4) In advanced prostate cancer, blood levels of testosterone don’t always correlate with testosterone levels inside the cancer cell. Meaning, just because a drug lowers blood testosterone levels, which doctors typically measure, that doesn’t mean the drug is lowering testosterone in the cancer cell where it matters!
5) Advanced prostate cancers cells mutate and start to lose their ability to produce prostate specific antigen (PSA), which doctors measure blood levels to see if an anti-cancer drug is working or not. The problem is that as the tumor cells mutate and lose their ability to produce PSA, doctors can be fooled into thinking that a drug is working when it is not. For example, a PSA level may be 0.5 ng/mL, but on PET scan, there are metastases everywhere.
There is a lot to learn about the nuances of advanced prostate cancer. Educating others is what I hope to accomplish in this series of newsletters. I promise not to make it all doom and gloom. In fact, it is my hope that the ending will surprise everyone. In a good way:)